Get ready for the era of the readmission rates.
While in the past this metric was simply useful, it’s quickly becoming an essential KPI that represents the ideals of a new era of value-based healthcare. This simple concept is moving to the forefront in multiple areas, so through this article, we want to help you understand some of the most important points around it including
- What’s driving the new attention to readmission rates
- Major factors around the metric in hospital settings
- How Medicare is addressing them
- News of organizations that aren’t measuring up to the new standards
- Advice on how to improve rates at your facility
Why The Recent Emphasis?
Readmission rates have long been a trusted measure of effective and responsible care, but only since the Affordable Care Act (ACA) of 2010 established the readmission reduction program (effective October 1, 2012) did it become a primary assessment driver in the industry.
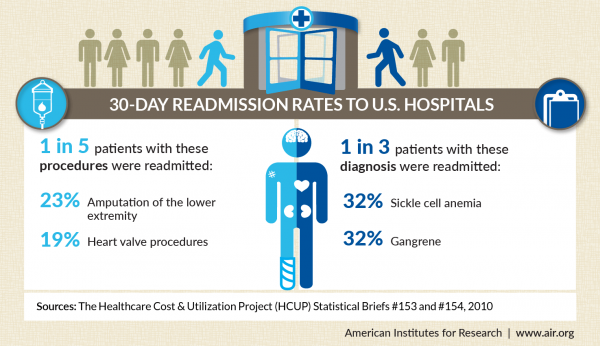
The program was specifically designed to incentivize hospitals to take strategic action in reducing expensive and unnecessary hospital readmissions. CMS defines these readmissions as “an admission to a subsection(d) hospital within 30 days of a discharge from the same or another subsection(d) hospital.” At the time of implementation, Medicare was seeing a readmission rate of 20% of its hospital patients within one month of being discharged, a rate CMS decided was excessive.
![]()
In response, CMS decided to begin a payment reduction program that directly impacted hospital reimbursements for readmissions. The agency began by deducting 1 percent of every Medicare payment for hospitals that have been determined to have excessive readmissions, but in October of 2013, the rate was increased to 2 percent and pushed again to 3 percent in 2014. CMS has found that the program has been somewhat effective in preventing avoidable readmissions — the national readmission rate for Medicare facilities had dropped to below 18 percent by 2013.
A focus on readmission rates is about more than just saving CMS a few dollars though. A study by the School Of Public Health found that the Veterans Administration could save $2,140 per patient just by taking measures to ensure that patients at high risk of readmission were properly handled.
Beyond the government sector, studies have found that 15 to 25 percent of people discharged from a hospital will be readmitted within 30 days or less and that a large number of those readmissions are preventable. From a patient perspective, reducing readmissions also makes for better community relations and increases hospital brand trust.
FierceHealth Finance reports that readmissions cost hospitals $41.3 billion between January and November of 2011. $24 billion of that fell to Medicare, $7.6 billion to Medicaid, and $8.1 billion to privately insured patient readmissions. Uninsured visits accounted for $1.5 billion and 200,000 patients.
In an era of value-based care, patients returning to facilities to be treated for conditions and issues that were improperly addressed on their initial interaction with a caregiver is a cardinal sin. Wasted clinical resources and squandered patient time and energy will not be as easily written off going forward as they have been in the traditionally fee-for-service world of U.S. healthcare.
What Causes Hospital Readmission Rates
Addressing the problem of unnecessary readmissions cannot be separated from an examination of the causes and perhaps surprisingly, when it comes to hospitals, one of the biggest causes is simple — communication.

A study presented by the Harvard Business Review found that on average, a hospital could reduce its readmissions rates by 5% if it simply prioritized communication with patients while also complying with evidence-based standards of care. Unfortunately, motivating clinicians to move on to “softer” communications-based initiatives has proven difficult. An HCAHPS (Hospital Consumer Assessment Of Health Providers And Systems) survey in 2006 found that only 71 percent of the survey respondents would rate their hospital experience as high. This is significant because the survey dealt directly with questions of communication including
- Recovery instructions
- Quality of caregiver communications
- Caregivers’ ability to respond to patients’ explicit needs (i.e., calls for help)
Harvard went as far as to test which of two factors (between communications and response) had the biggest impact on HCAHPS scores (along with the process of care measures.) This is important because improving these two indicators required very different resources…response-focused issues require investments in things and technologies (including RFID location systems and visual monitoring systems) while the communication-focused issues point to cultural questions that are best addressed through initiatives such as training programs to teach interpersonal skills and empathy to caregivers in a facility.
The researchers examined the relationship between the two dimensions of the patient experience, supplemented with analysis of 5 in-depth case studies of acute-care hospitals involving around 50 semi-structured interviews with administrators, nurses, and physicians. The results indicated that when process-of-care quality is high, then communication-focused efforts have a much stronger effect on reducing readmissions compared to improving focused response factors. According to the study,
“The communication-focused dimension and process-of-care combo results in a 5-percentage-point reduction in 30-day readmission rates for an average U.S. hospital. The reduction is just under three percentage points for the response focus and process of care combo. The net difference of over two percentage points for an average hospital is a conservative estimate and compares results for only a 1% increase in each patient experience dimension.”

Additionally, distinct patterns exist around. Medicare found that its patients accounted for more than 55% of all readmissions and 58.2% of all costs associated with readmissions. The top five readmission conditions in 2011 were
- Congestive heart failure, non-hypertensive (134,500, 30-day readmissions)
- Septicemia, excluding labor (92,900)
- Pneumonia, excluding that caused by STIs or tuberculosis (88,800)
- Chronic obstructive pulmonary disease and bronchiectasis (77,900)
- Cardiac dysrhythmias (69,400)
Less impactful, but still notable were the numbers of Medicaid patients. They were found to account for 20.6% of all readmissions and take credit for 18.4% of associated costs. Their most common readmissions were
- Mood disorders (41,600)
- Schizophrenia and other psychotic disorders (35,800)
- Diabetes mellitus with complications (23,700)
- Complications of pregnancy, not including early or threatened labor (21,500)
- Alcohol-related disorders (20,500)
Examining the causes of readmission rates on regional, population, and individual facility levels are essential to addressing the readmission problem overall and tackling any reimbursement issues that a facility may encounter.
Medicare’s New Quality Measure For Readmission Rates
Medicare is constantly refining measurement standards around admission rates and one of the latest addresses readmissions for heart failure.
The Hospital Inpatient Quality Reporting (Hospital IQR) program authorizes CMS to pay hospitals for successfully reporting certain quality measures at a higher annual update to their designated reimbursement rates. The program, which was established in the Medicare Prescription Drug, Improvement, and Modernization Act (MMA) in 2003 and additionally provides CMS with data, meant to aid healthcare consumers in their decisions.

Just this month, CMS concluded the trial for a new claims-based measurement for readmission of heart failure patients. The measurement, of excess days in acute care (EDAC) will be formally included as a quality metric in the fiscal year 2018.
According to The Hospitalist, CMS hopes that the measure will serve as a tool to educate both hospitalists and hospitals about 30-day post-discharge outcomes for patients with heart failure as well as improve understanding of the services utilized, all in the hopes their efforts will translate to improved interventions. According to CMS spokesperson Alper Ozinal, hospitalists are frequently left in the dark after a patient leaves their facility and receive “little feedback about what happens to their patients after discharge.”
Ozinal continued, “CMS found substantial variation in utilization across hospitals, which suggests an opportunity for improvement in transitional care practices. CMS anticipates that the measure will support hospital efforts to further optimize the quality of care, particularly the quality of transitional care, by providing a more comprehensive picture of post-discharge events.”
The trial run of the measure began on September 8 of this year, focusing on Medicare fee-for-service patients age 65+ who had been hospitalized under a principal discharge of heart failure. Their outcomes are risk-adjusted for comorbidities, age, and sex. The results will be posted in a report on the QualityNet website, and CMS welcomes comments.
Organizations Failing The Readmission Test
As the focus on readmission continues, we’re beginning to see impact unfold and it’s not all pretty.
Just last month, 5 Montana hospitals were penalized for high readmission rates. CMS identified the following facilities as having excessive reimbursement rates according to NBC Montana:
- St. James Healthcare, Butte
- St. Peter’s Hospital, Helena
- Benefits Healthcare, Great Falls
- Northern Montana Healthcare, Havre
- St. Vincent Healthcare, Billings
All five facilities will be subject to penalties under Medicare for their readmission rates between October 1, 2014, and September 30, 2015. It’s worth noting that several of the hospitals had penalties prior to the fiscal year in question, but some of them have been taking action.
St. James Healthcare officials have been implementing post-discharge phone calls to patients within the first 48 hours of leaving the hospital, along with early physician follow-up post-hospitalization and improving medication instruction at discharge. According to a hospital representative,
“Readmissions are a serious issue and one that we’ve taken extensive measures to address. While our readmission rates are consistent with the national average, even one is too many, and we are committed to bringing these rates down to zero.”
Thanks to their work, they’re already seeing improvements, and the community is taking notice. Residents are expressing relief that the people they trust with their health are doing their work right the first time. This kind of positive perception is essential in maintaining open communication with patient communities.

It’s important to remember that high readmission rates aren’t only a concern of CMS. Insurance companies track this metric too and have their methods of addressing the problem — something we see an example of in Minnesota.
According to the Post Bulletin, insurer Medica/Optum has confronted a chain of child and adolescent psychiatric clinics around readmission rates they’ve deemed as being too high. Medica/Optum is suggesting that children being treated at PrairieCare on an inpatient basis are being re-hospitalized at a rate 3x that of children treated by other providers, in addition to their initial stays being longer than necessary.
Medica/Optum has provided data across a 12-month period demonstrating that children treated at the PrairieCare facility were readmitted to a hospital within 90 days of discharge 42 percent of the time. The average for other facilities in the area is 15.5 percent. The adolescent readmission rate showed a similar, though less severe problem with a readmission rate of 18.6 percent versus 15.5 percent.
The facility has responded with a rejection of the data. According to PrairieCare President Dr. Stephen Setterberg, “In these situations there are statistics, and there are lies, and sometimes it’s tough to know the difference.”
The PrairieCare dispute highlights one of the most challenging aspects of the readmission issue: In traditional fee-for-service environments, facilities are under pressure to keep stays as short as possible. Todd Archbold, chief development officer for PrairieCare, sees this as the issue with Medica/Optum,
“They’re approving fewer days, and they’re giving a lot of pressure to our psychiatrists to discharge patients and get them out of our programs much sooner than we feel medically reasonable…The average length of stay in our program has been 9.4 days for adolescents which is exactly the national average…Our length of stay in all our programs have been spot on with the national average.”
We can expect to continue to see these types of conflicts as value-based initiatives collide with historical fee-for-service environments.
Reducing Readmission Rates At Your Facility
Even if you haven’t yet been alerted to a readmission problem by a payor or government entity, it’s worth not only tracking the metric yourself, but also implementing procedures to bring your rates in alignment with, or to a better level than accepted standards. Here are a few suggestions to get started.
Follow-up Phone Calls
This simple, low-tech solution can be incredibly powerful.
Contacting discharged patients by telephone for questioning can be incredibly effective in reducing readmissions, especially in high-risk populations. Take the example of St. Elizabeth Medical Center in New York who cut their rates by 56 to 75% by implementing a calling program that involved multiple, automated calls in the month following discharge.

A More Efficient Handoff Process
As the patient is transitioning out of your facility, make sure to take advantage of the opportunity to communicate with them and ensure they fully understand their care responsibilities. HealthLeadersMedia suggests shifting your perspective on the transition and making them standard, measurable processes that can be tracked across different providers (hospitals, rehab facilities, skilled nursing facilities, homes, etc.) in the care cycle.
Tools like ReferralMD’s referral management and patient access tools can help keep the referring provider and patient in the loop at all times.
Collaborative Programs
Sometimes partnering up can bring big benefits.
Hospitals in Michigan implemented a program designed to increase 7-day follow-up rates post-discharges. They worked together over a 1-year period, submitting assignments and participating in quarterly telephone conferences, meetings, and Web-based events. A group of researchers compared the results of the participating hospitals and nonparticipating facilities. They found that the program resulted in a larger decrease in readmission rates for participating hospitals (29% vs. 27.3%) than for nonparticipating (26.4% vs. 25.8%.)
Implementing Technology
While improving readmission rates will rely heavily on improving personnel habits and communicating with patients, it’s important not to forget the benefits that technology provides.
Telehealth and telemedicine allow for communication with patients on a regular basis after discharge. Advanced data analytics can give you insight into the populations (cardiac patients, the elderly, the homeless, etc.) that have the greatest issues with readmissions as well as causes and solutions. Patient Portals can serve as an excellent touch-point for information resources and feedback from patients after they’ve been discharged, and SMS/text messaging options can help patients stay on top of their medication, wound care, and other post-discharge responsibilities.
Hospital readmissions reduction can be a complex issue, but with proper communication with patients and other caregivers, you can get a jump on addressing facility issues before they begin and without the intervention of an outside party. Make sure you are taking advantage of your existing referral network to reduce readmission and try out our physician network management solutions today.
Related Posts


Subscribe to Our Blog
Recent Posts